




The morning or evening administration of antihypertensive medication had no effect on blood pressure levels measured by 24-hour ambulatory blood pressure monitoring (ABPM) or on quality of life in the HARMONY study. The results of the open-label, randomized, cross-over trial were presented by Neil R. Poulter, MD, Imperial College London, United Kingdom.
The optimal timing of administering antihypertensive therapy is the subject of clinical studies because of data suggesting that nighttime, versus daytime, blood pressure levels are a better predictor of major adverse cardiovascular events (MACE). Data from randomized, controlled trials have also suggested that at least some nighttime dosing of antihypertensive medication provides better cardiovascular protection. The HARMONY trial was designed to compare the impact of morning or evening dosing of antihypertensive medication on 24-hour ABPM.
In HARMONY, men and women aged 18-80 years who had stable and well-controlled blood pressure (defined as ≤150 mmHg systolic and ≤90 mmHg diastolic) for ≥3 months while taking ≥1 antihypertensive medication were randomized to taking their medication in the morning (between 6 and 11 am) or in the evening (between 6 and 11 pm). At 12 weeks, without a washout period, patients were crossed over to taking their medication at the other time period. All patients took their usual antihypertensive therapy. There was a 50:50 randomization of patients in London and Thessaloniki, Greece.
Evaluations were conducted at baseline, randomization, the 12-week crossover, and the end of the 24-week study. Parameters included were heart rate and clinic blood pressure at each evaluation, 24-hour ABPM at baseline, 12 weeks, and 24 weeks, and quality of life by questionnaire at 12 weeks and 24 weeks. Adverse events and adherence to therapy were evaluated at 12 weeks and 24 weeks.
A total of 103 patients were randomized during the recruitment period of July 2013 and January 2015, of whom 95 (92%) patients completed all ABPM evaluations.
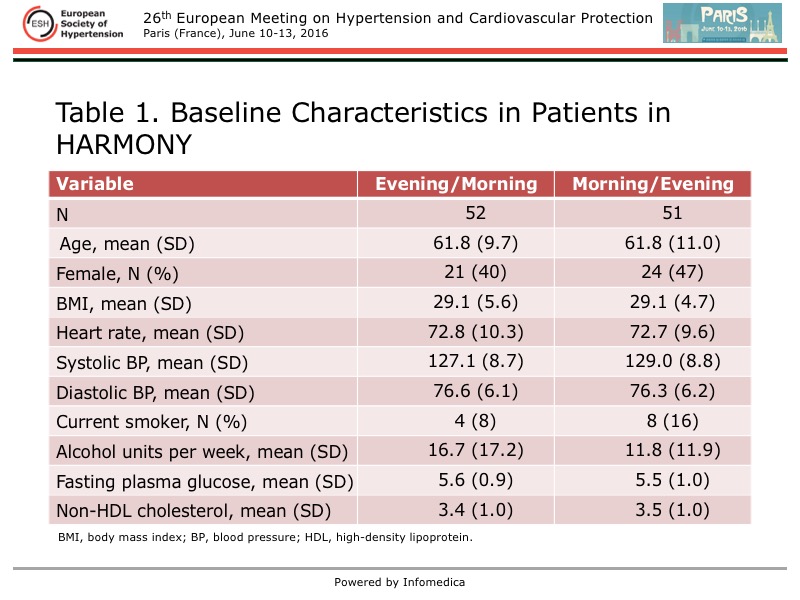
The mean age of the patients was 62 years and 44% were women. The baseline characteristics were similar between the groups and reflected a typical overweight, hypertensive population (Table 1). The levels of fasting glucose levels and non-high-density lipoprotein cholesterol were typical for the patient population. The smoking rates were low. As required by the study protocol, systolic and diastolic blood pressure were well controlled.
{kind=link}
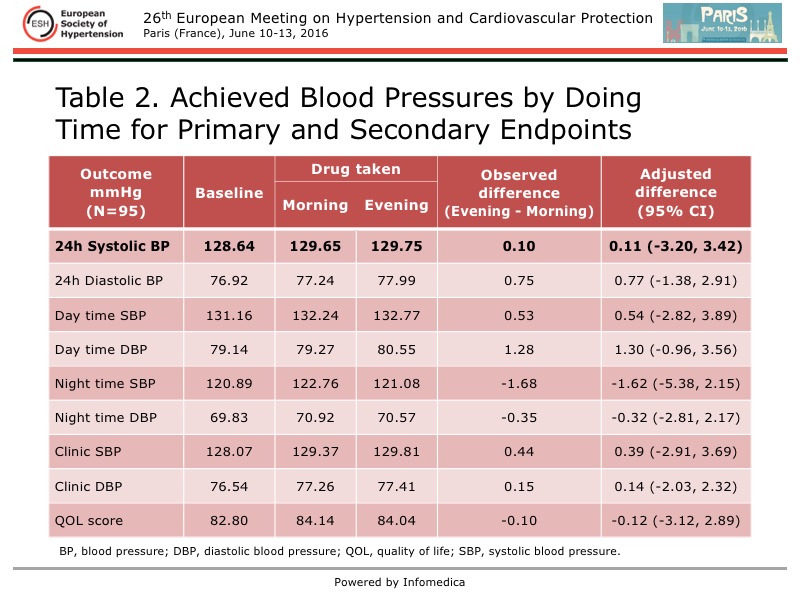
The primary endpoint of the mean 24-hour systolic blood pressure measured by ABPM was the same regardless of whether the antihypertensive medication was taken in the morning or the evening (Table 2). The observed difference between taking the medication in the evening rather than the morning was only 0.10 mmHg.
{kind=link}
Likewise, no differences were seen for any of the prespecified secondary endpoint (Table 2). The largest between-group difference was seen for nighttime systolic blood pressure, with a reduction of 1.68 mmHg with the drug taken in the evening versus the morning. Although this was not statistically significant within the HARMONY study, Poulter noted that at a population level this could be important in relation to cardiovascular events. Overall, no signal was observed for a benefit of taking the antihypertensive medication in the evening rather than the morning.
Quality of life was not impacted by the timing of therapy, as captured by the self-reported questionnaires. The results were similar for the subgroups of age, sex, and country.
There was a normal distribution of the individual differences in the 24-hour systolic blood pressure. Although 7 patients were outliers in this distribution, with quite large differences between morning and evening dosing, a sensitivity analysis showed this had no impact on the study results.
The ongoing Treatment in Morning versus Evening (TIME) trial with some 10,200 patients followed for 5 years is anticipated to provide definitive evidence of whether or not there is a benefit to dosing antihypertensive medications in the evening to provide better protection against MACE [Rorie DA et al. BMJ Open 2016].