




The clinical relevance and the mechanisms of orthostatic hypertension (OH) are not fully understood or appreciated. Yet, evolving research has demonstrated cardiovascular (CV) morbidity and mortality associated with OH, stated Jean-Jacques Mourad, MD, CHU Avicenne, Bobigny, France. Further research is required to determine whether OH is a risk factor or a risk marker of CV disease, and whether OH plays an independent role in specific populations.
During normal standing, gravitational redistribution of about 500-1000 ml of circulating blood in the veins located under the diaphragm results in reductions in venous return and stroke volume, thereby inducing reflex responses that increase sympathetic activity and reduce vagal activity, and ultimately leads to maintenance of blood pressure levels, without variation, to the level similar to that when seated.
A pioneering publication in 1985 first described OH. Excessive venous pooling that lead to a decrease in cardiac output that resulted in an increase in sympathetic activity and diastolic blood pressure (DBP) was found in patients with a DBP <90 mmHg when seated but >90 mmHg when standing [Streeten DH et al. Hypertension 1985].
Since then, the definition of OH has been evolving. The most recent definition is an increase in systolic blood pressure (SBP) ≥20 mmHg when assuming an upright position (head-up tilting to 70 degrees within the study) from the supine position or a ≥20 mmHg increase in SBP after standing [Kario K et al. J Am Coll Cardiol 2002].
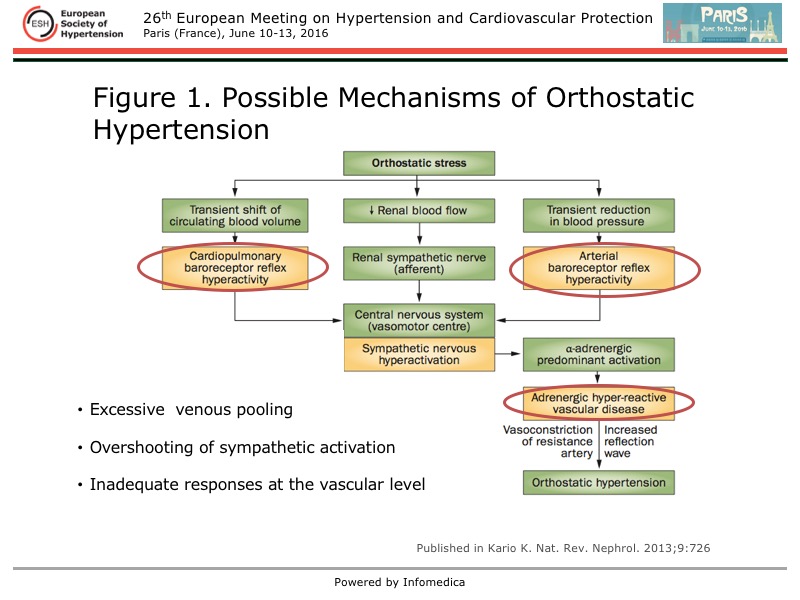
Presently, the mechanisms of OH are unclear, and they may differ between patients who are young and elderly, who have systolic rather than diastolic hypertension, or are normotensive versus (treated or untreated) hypertensive. Kario and colleagues have proposed that patients with OH have excessive venous pooling with an overshooting of sympathetic activation and an inadequate response at the vascular level (Figure 1).
{kind=link}
OH is a feature of essential hypertension in the elderly and in persons with abnormal diurnal variation (extreme dipping), and in type 2 diabetes [Fessel J, Robertson D. Nat Clin Pract Nephrol 2006]. In some populations, including the elderly and diabetes, the prevalence of OH can reach 20%.
Yet, OH is not a benign condition. Kario and colleagues first demonstrated a link between silent cerebrovascular disease and standing OH in elderly patients with hypertension [Kario K et al. J Am Coll Cardiol 2002]. In the control group (n=192), the rate of events was 1.4 per person, compared with 3.4 per person in the OH group (n=26; p<0.0001) and 2.7 per person in the orthostatic hypotension group (n=23; p=0.04). A higher prevalence of multiple lesions was found in patients with OH and orthostatic hypotension.
The prospective, observational ARIC (Atherosclerosis Risk in Communities) cohort study confirmed the association between orthostatic increases and decreases in SBP and brain lesions [Yatsuya Y et al. Hypertension 2011]. The prevalence of OH was 2.4% amongst the nearly 13,000 patients, with an average age of 55 years.
A decline in cognitive function in association with OH was found in a study of 334 community-dwelling adults aged ≥75 years (mean age 80 years) [Matsubayashi K et al. Stroke 1997]. A rise of ≥20 mmHg in SBP was significantly related with a decline in a number of measures of cognitive function, and a higher rate of lacunar lesions compared with postural normotension (3.5 vs 2.1) and more advanced periventricular hyperintensities.
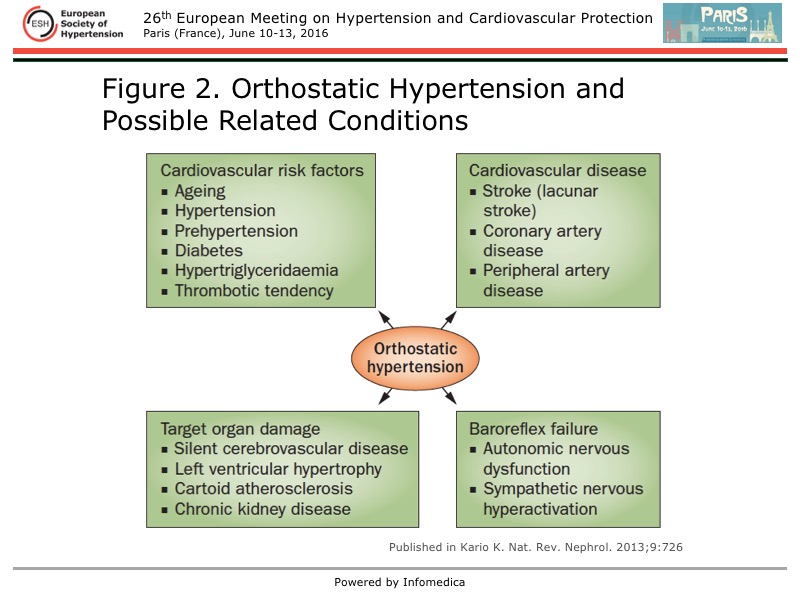
OH is a component of blood pressure variability patterns that are linked to CV morbidity and mortality (Figure 2).
{kind=link}
Two studies have demonstrated an association between OH and hard CV events. An adjusted risk for all-cause mortality of 1.23 (p=0.03) and CV mortality of 1.41 (p=0.02), compared with orthostatic normotension, was found in the observational Pro.V.A. study [Veronese N et al. Am J Hypertens 2015]. This study included 3,099 participants aged ≥65 years (mean age 75 years) in Italy, and found a 26% prevalence of OH.
An increased risk of CV morbidity and mortality was found with OH versus orthostatic normotension (hazard ratio [HR], 1.51; p=0.0085) in the 2-year follow-up of the PARTAGE (Predictive Values of Blood Pressure and Arterial Stiffness in Institutionalized Very Aged Population) study [Agnoletti D et al. Hypertension 2016]. The mean age of the 972 participants was 88 years, and most (76%) were women. After adjustment for age, sex, body mass index, Charlson Comorbidity Index, and heart failure, OH remained an independent risk factor (HR, 1.51; p=0.01). Risk prediction was improved with OH in the PARTAGE study.
Whether OH is a therapeutic target requires further research. Kario and colleagues showed benefit with alpha-blockade. Doxazosin 1-4 mg dosed at bedtime was beneficial for controlling OH evaluated with home blood pressure monitoring [Hoshide S et al. Hypertens Res 2012].
Evidence suggesting OH is an independent marker of CV morbidity and mortality requires confirmation from further research. Work is also needed for an agreed definition of OH, and define optimal treatment.